









Awọn itọju iṣoogun fun hyperplasia prostatic alailẹgbẹ
Mild, stable symptoms may only be monitored clinically at the time of the annual medical examination.
Awọn elegbogi
Alphabloquants. Alpha blockers help relax smooth muscle fibers in the prostate and bladder neck. This improves the bladder emptying with each urination, reducing frequent urges to urinate. The alpha blocker family includes tamsulosin (Flomax®), terazosin (Hytrin®), doxazosin (Cardura®) and alfuzosin (Xatral®). Their degree of effectiveness is comparable. The benefits are felt quickly, after 1 or 2 days of treatment. Some of these drugs were originally used to treat hypertension, but tamsulosin and alfuzosin specifically treat benign prostatic hyperplasia.
Some of these drugs can cause dizziness, fatigue, or low blood pressure. Low blood pressure can also occur if alpha blockers are used at the same time as erectile dysfunction drugs (sildenafil, vardenafil, or tadalafil). Discuss it with his doctor.
5-alpha-reductase inhibitors. These types of drugs, of which finasteride (Proscar®) and dutasteride (Avodart®) are part, reduce the production of dihydrotestosterone. 5-alpha-reductase is a hormone that converts testosterone into its active metabolite, dihydrotestosterone. The maximum effectiveness of the treatment is observed 3 to 6 months after the start of the medication. There is a decrease in the volume of the prostate of about 25 to 30%. These drugs cause erectile dysfunction in about 4% of the men who take them. Increasingly, they are used in conjunction with alpha blockers.
awọn akọsilẹ. Finasteride significantly reduces the risk of developing prostate cancer, according to a large study conducted in 2003 (the Prostate Cancer Prevention Trial)7. Paradoxically, in this study, the researchers noted an association between taking finasteride and a slightly more frequent detection of a severe form of prostate cancer. The hypothesis that finasteride increases the risk of serious prostate cancer has since been refuted. It is now known that the detection of this form of cancer was facilitated by the fact that the size of the prostate had decreased. A smaller prostate helps detect tumors.
Pataki. Make sure that the doctor who interprets the prostate antigen blood test (PSA) is aware of treatment with finasteride, which lowers PSA levels. To find out more about this screening test, see our Prostate Cancer fact sheet.
Combined therapy. Treatment consists of taking an alpha blocker and a 5-alpha-reductase inhibitor at the same time. The combination of the 2 types of drugs would be more effective than one of them in slowing the progression of the disease and in improving its symptoms.
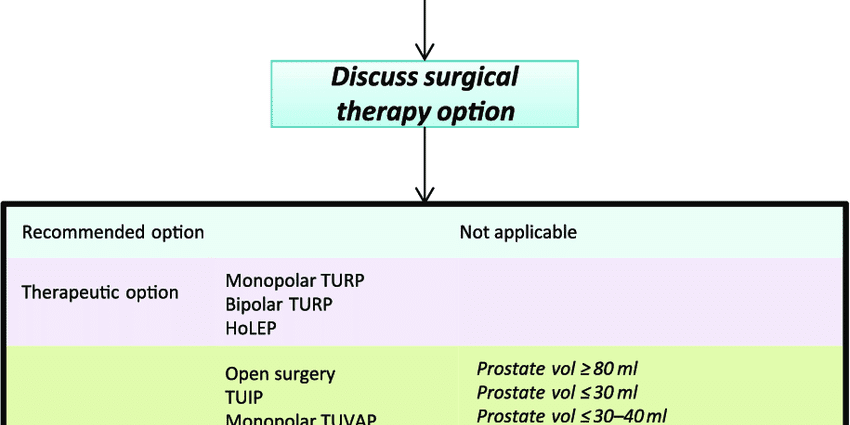
Awọn iṣẹ abẹ
If drug treatments do not bring improvement, surgical treatment may be considered. From the age of 60, 10 to 30% of patients resort to surgical treatment to relieve the symptoms of benign prostatic hyperplasia. Surgery may be necessary in the event of complications.
Transurethral resection of the prostate or TURP. This is the intervention most frequently undertaken, due to its good effectiveness. An endoscopic instrument is introduced through the urethra to the bladder. It allows curettage of the hyperplasied parts of the prostate. This operation can also be carried out using a laser.
Almost 80% of men who undergo this procedure then have a ejaculation retrograde : instead of being ejaculated, the sperm is directed into the bladder. Erectile functions remain normal.
Awọn akọsilẹ. Besides TURP, other, less invasive methods can destroy excess prostate tissue: microwaves (TUMT), radiofrequencies (TUNA) or ultrasound. The choice of method depends among other things on the amount of tissue to be removed. Sometimes thin tubes are placed in the urethra to keep this duct open. The operation is performed under regional or general anesthesia, and lasts about 90 minutes. From 10% to 15% of operated patients may have a second surgery within 10 years of the operation.
Transurethral incision of the prostate or ITUP. The indicated operation for mild hypertrophy is to widen the urethra by making small incisions in the neck of the bladder, instead of reducing the size of the prostate. This operation improves urination. It carries little risk of complications. Its long-term effectiveness remains to be proven.
Open abẹ. When the prostate is large (80 to 100 g) or complications require it (recurrent periods of urine retention, kidney damage, etc.), open surgery may be indicated. This common surgical operation is done under anesthesia and involves making an incision in the lower abdomen to remove part of the prostate gland. This procedure can cause retrograde ejaculation, as is the case with transurethral resection. Another possible side effect of the operation is urinary incontinence.